



Portland, OR Mindfulness-Based Recovery: Heal Trauma

Key Takeaways
- Portland's co-occurring caseloads require mindfulness programs built for trauma from the start, since PTSD and SUD overlap heavily and standard MBRP was not originally designed for active PTSD symptoms 1, 6.
- MBRP shows its strongest evidence for craving, withdrawal, and distress tolerance across nine RCTs with 901 participants, while trauma-integrated adaptations remain promising but await confirmatory studies 12, 5.
- Local delivery varies widely: VA Portland's Mindfulness Institute embeds groups within SATP for veterans, while non-veterans rely on community IOPs, CHAT/MOUD handoffs, and TriMet-accessible schedules 3, 10, 11.
- Before referring, compare whether the IOP uses manualized MBRP, addresses dissociation and hyperarousal during silent practice, sequences care concurrently with trauma-focused work, and accepts warm handoffs 12, 6, 1.
Why Mindfulness Earned a Seat at the Co-Occurring Table
If you're placing individuals with dual diagnoses into Portland-area programs, you understand the complexity. Trauma histories and substance use rarely present neatly, and those most in need of care often have fragmented treatment records. The question isn't if mindfulness belongs, but what role it plays.
Consider the epidemiology that influenced VA guidelines. A national study cited in current VA co-occurring guidance found that 44.6% of individuals with lifetime PTSD also met criteria for an alcohol use disorder or substance use disorder, and PTSD was associated with a significantly higher likelihood of an SUD diagnosis 1. This substantial overlap represents the population many Portland IOPs treat, regardless of how it's documented.
This context is crucial. Mindfulness-based recovery in Portland cannot be designed for single-diagnosis clients and then retrofitted for trauma. The clinically sound approach is to build programs for co-occurring presentations first, then determine how mindfulness-based interventions can lead, augment exposure-based work, and where caution is still warranted. This article explores that approach.
The MBRP Evidence Base, Read Without Rose-Colored Glasses
What Nine RCTs and 901 Participants Actually Show
Before your next referral conversation, consider this evidence: a peer-reviewed synthesis of nine randomized controlled trials (RCTs) of Mindfulness-Based Relapse Prevention (MBRP), involving 901 participants, found significant differences favoring MBRP for withdrawal and craving outcomes compared with control conditions 12. The authors propose a mechanism: mindfulness practice appears to reduce activity in craving-related brain circuits while strengthening self-regulation networks, which are crucial when individuals encounter cues that trigger old behaviors 12.
The strongest signal isn't solely about abstinence rates, but about the internal processes that precede substance use: craving intensity, distress tolerance, and the interval between a cue and a choice. These are the outcomes MBRP most reliably influences, and they are precisely what individuals with co-occurring conditions struggle with in early recovery, especially when trauma symptoms are pronounced and reactivity is high.
This framing impacts how a client's week is structured. For individuals in a Portland IOP, MBRP's evidence supports its use as a core modality for regulating urges and arousal, not merely as a supplementary wellness activity. When a program presents mindfulness as a stress-reduction accessory, it underestimates the trial findings. When it describes it as a relapse-prevention discipline with a defined curriculum, consistent practice requirements, and clinical supervision, it aligns more closely with the evidence 12.
Trauma-Integrated MBRP: Promising, Not Yet Settled
Standard MBRP was not initially designed for individuals with PTSD, a significant consideration given that over 90% of women in some SUD treatment samples report histories of physical or sexual trauma 6. Trauma-Integrated MBRP (TI-MBRP) is an adaptation that incorporates psychoeducation and elements from Cognitive Processing Therapy into the standard MBRP curriculum. This addresses avoidance, shame, and trauma-linked cognitions alongside core mindfulness practices 6.
A 2022 randomized trial comparing TI-MBRP with standard MBRP in women with co-occurring PTSD-SUD yielded results that warrant careful interpretation. Both MBRP conditions reduced PTSD and substance use symptoms, indicating that even the standard protocol impacted trauma symptoms in this population. The authors concluded that"MBRP alone may be effective in reducing both PTSD and SUD symptoms in women with PTSD-SUD; however, confirmatory studies are warranted"5.
The need for confirmatory studies is a crucial point often overlooked by clinicians. A single community-setting RCT provides an initial signal, but not a definitive evidence base. If you refer an individual with active PTSD to a program using TI-MBRP, view it as a defensible clinical choice with promising early data, not as a replacement for exposure-based work that some individuals may still require. If a program uses MBRP without trauma-informed adaptations for a co-occurring caseload, inquire about their approach to dissociation, hyperarousal during silent practice, and the pacing decisions necessitated by these symptoms 6.
Where the Evidence Gets Mixed
Broadening the scope to the general mindfulness-based intervention literature reveals a less clear picture. A 2021 systematic review and meta-analysis of MBIs for substance use disorders concluded that"MBIs have been examined for the treatment of SUDs, but available evidence is mixed,"noting that heterogeneity across interventions, populations, comparators, and outcome measures makes precise effect sizes difficult to determine 7.
For referral purposes, this means MBRP, when delivered as a structured 8-week protocol with fidelity, has more robust data supporting it than the broader category of "mindfulness in SUD care" 7. When evaluating a Portland program, this distinction is worth asking about directly. A weekly guided-meditation group led by various facilitators is a different intervention than a manualized MBRP course with trained clinicians and a defined practice progression, even if both are labeled "mindfulness" in intake materials.
Sequencing Mindfulness With Trauma-Focused Work
The Old Sobriety-First Debate Is Over
The 2023 VA/DoD Clinical Practice Guideline for PTSD and the 2021 VA/DoD Clinical Practice Guideline for SUD jointly recommend that evidence-based treatments for both disorders be offered concurrently, rather than sequentially based on sobriety milestones 1.
This resolves a debate that may still arise in intake meetings. The older sequential model, which prioritized stabilizing substance use before addressing trauma, was based on cautions not supported by current evidence. Integrated, trauma-focused interventions that address both disorders offer greater benefits compared to treatment-as-usual or non-trauma-focused approaches 1.
For mindfulness sequencing, this means MBRP does not need to be delayed until an individual achieves a sobriety benchmark, nor does Prolonged Exposure or CPT need to be deferred until mindfulness curriculum completion. The focus shifts from "when do we allow trauma work" to "which modality is serving which purpose this month," providing a more practical framework.
When Mindfulness Leads, When It Augments
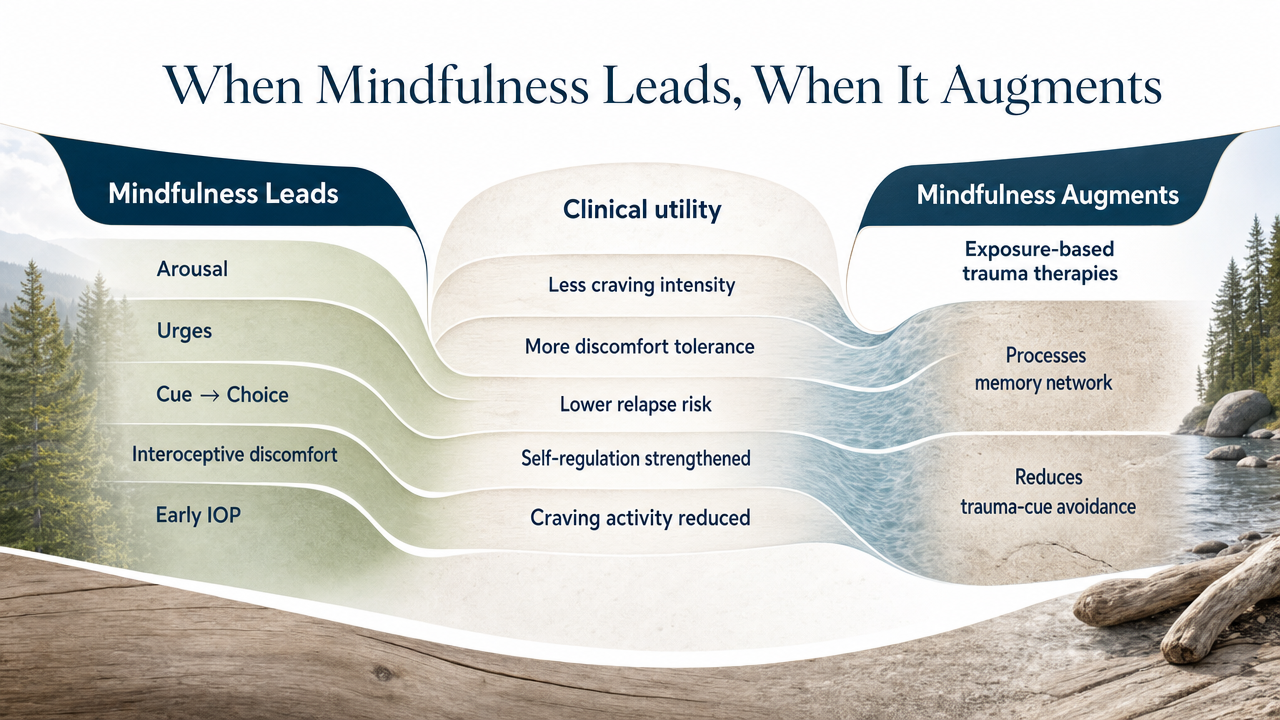
Consider mindfulness-based recovery in terms of its specific clinical utility. The synthesis of nine MBRP RCTs involving 901 participants indicates a distinct effect profile: reductions in craving intensity, improved psychological discomfort tolerance, and lower relapse risk. This is linked to a plausible mechanism where mindfulness reduces craving-related brain activity while strengthening self-regulation 12. This differs from exposure-based trauma therapies, which primarily process the memory network itself and reduce avoidance behaviors related to trauma cues.
The sequencing logic becomes clearer: mindfulness takes the lead when the immediate clinical challenge involves arousal, urges, and the brief interval between a cue and a choice. Early in an IOP program, when an individual is learning to tolerate interoceptive discomfort without resorting to substances, MBRP is highly valuable. It is also a modality likely to keep individuals engaged during challenging middle weeks, as skills are practiced daily, not just during sessions.
Mindfulness augments when the primary focus is trauma processing. Prolonged Exposure and CPT address aspects that MBRP does not; they facilitate the processing of trauma memories, not just the reactivity surrounding them. During these weeks, mindfulness practice supports exposure work by providing individuals with reliable ways to regulate between sessions and integrate what emerges. While the 2022 TI-MBRP trial suggests that trauma-integrated MBRP can reduce PTSD symptoms independently for some women with co-occurring PTSD-SUD 5, until confirmatory studies are available, consider this a promising avenue rather than a replacement for exposure-based work when clinically indicated.
In practical terms, do not expect mindfulness to perform the role of trauma processing, nor exposure therapy to manage cravings. Sequence interventions based on their function, not on loyalty to a particular modality.
Clinical Sequencing at a Glance
Here's a quick reference for treatment planning meetings:
| Clinical Target | Mindfulness Role | Typical Pairing | Evidence Anchor |
|---|---|---|---|
| Craving intensity, urge surfing, cue reactivity | Leads | Relapse prevention skills, MAT where indicated | 9-RCT MBRP synthesis, 901 participants 12 |
| Distress tolerance, emotion regulation in early recovery | Leads | DBT skills groups | MBRP mechanism data 12 |
| PTSD symptoms in women with co-occurring SUD | Leads or co-leads | Seeking Safety, CPT elements | 2022 TI-MBRP RCT, confirmatory studies pending 5 |
| Trauma memory processing, avoidance reduction | Augments | Prolonged Exposure, CPT | VA/DoD integrated care guidance 1 |
| Between-session regulation during exposure work | Augments | Any trauma-focused protocol | MBRP self-regulation findings 12 |
This table offers a framework for considering each modality's role in different phases of care, rather than a rigid prescription.
Real Recovery Starts in Portland, Oregon
Call now or verify insurance to take the first step toward lasting recovery in Portland.
Portland's Delivery Infrastructure for Trauma-Informed Mindfulness
VA Portland's Mindfulness Institute Inside SATP
For veterans, VA Portland Health Care operates its Mindfulness Institute as a clinical service, not merely a wellness offering. The Institute provides multi-week mindfulness and self-compassion groups, chronic pain and stress programs, and, importantly, mindfulness groups integrated directly within the Substance Abuse Treatment Program (SATP) 3. This integration means the practice curriculum runs concurrently with the SUD treatment plan, aligning with co-occurring evidence-based recommendations.
The Institute describes its work as a"trauma-informed mindfulness program designed to re-train the brain to improve chronic health conditions, stress, and anxiety"3. This reflects a deliberate design choice, not just marketing. It indicates that facilitators pace silent practice, frame psychoeducation, and manage hyperarousal with a co-occurring caseload in mind, incorporating the specific adjustments advocated in the TI-MBRP literature 6.
Access is limited to those eligible for VA services. Non-veteran individuals in Portland require alternative pathways. For veterans with co-occurring PTSD and SUD, the SATP-embedded groups are a strong referral. For others, the Institute serves as a benchmark for what a robust trauma-informed mindfulness program entails, setting a standard for community programs.
Community IOPs, CHAT/MOUD, and the Field-Response Layer
Outside the VA, Portland's service delivery is more decentralized and has recently evolved. Portland Fire & Rescue's Community Health Assess and Treat (CHAT) team includes an Overdose Response Team and a Medication for Opioid Use Disorder (MOUD) pilot program. This initiative meets individuals at the scene of non-fatal overdoses, offers immediate buprenorphine, and connects them to follow-up recovery services. The program is explicitly framed as "an innovative, trauma informed approach" rather than a standard emergency department transfer 10. The MOUD pilot launched in February 2024 with City Council approval and funding through mid-2025 10.
This is relevant for mindfulness-based referrals because CHAT often represents the first clinical contact after an overdose. What occurs in the 72 hours following this contact significantly influences whether an individual reaches a community IOP. If the IOP you refer to can accept a warm handoff from a field-response encounter and initiate MBRP-style skills work within the first week—before craving windows disrupt the plan—a functional pipeline exists. If the IOP treats mindfulness as a later add-on, the timing is inappropriate for this population.
The Oregon Department of Veterans' Affairs also maintains a statewide behavioral health resource network offering peer-to-peer connections and crisis support, which is valuable for veteran clients who prefer not to enter through VA channels initially 4. Use this as a routing tool, not a substitute for clinical placement.
Access Realities: TriMet, MAX, and Continuity of Care
Continuity of care in an outpatient model heavily relies on transportation. Portland's transit system—TriMet buses, MAX Light Rail, the Streetcar, and the Aerial Tram—serves most neighborhoods where community IOPs and VA services operate. Frequent service and route-planning tools make three-times-weekly attendance feasible for individuals without personal vehicles 11. When evaluating a Portland program for someone dependent on transit, inquire about proximity to MAX lines and evening group schedules that accommodate return service.
The operational implication is subtle but critical. A trauma-informed mindfulness curriculum is effective only if the individual can attend. Session times that conclude after the last reliable evening bus implicitly exclude the very individuals who most need consistent care.
Underserved Populations and Culturally Responsive Practice
The equity argument for mindfulness-based recovery in Portland is a practical capacity issue, evident in the data. Analysis of electronic health record data from community behavioral health settings shows that the percentage of adult patients with a PTSD diagnosis increased from 24.6% in Q1 2019 to 31.6% in Q4 2022, with a significant rise in the odds of a PTSD diagnosis during that period 8. This seven-point shift in under four years is concentrated in settings where underserved individuals—including Native American communities, women with trauma histories, and those experiencing crisis—are most likely to seek care.
This trend means that individuals entering community IOPs today carry a greater trauma burden than those five years ago, and available modalities must be equipped to address this. Standard MBRP was not designed for this demographic profile. Trauma-integrated adaptations, however, were developed with this in mind; the TI-MBRP rationale explicitly highlights the over 90% trauma prevalence documented in women's SUD treatment samples 6.
Culturally responsive practice adds a dimension not fully addressed in mainstream MBRP literature. For Native American individuals, mindfulness-based work is often more effective when integrated with traditional wellness approaches, such as talking circles, elder-led practice, and culturally appropriate ceremonies, rather than replacing them with a secular curriculum. When screening a Portland program for an individual from a tribal community, ask directly how the mindfulness curriculum is framed and who delivers it. A trauma-informed program unable to articulate this distinction may not be adequately prepared for the caseload indicated by prevalence data 8.
What to Look For When Referring Into a Portland IOP
When evaluating a Portland IOP for an individual with co-occurring PTSD and SUD, the key question regarding mindfulness is not if it's offered, but how it's implemented. A concise screening checklist can streamline this process.
Inquire whether the mindfulness track is manualized. A structured 8-week MBRP curriculum with trained clinicians and a defined practice progression is distinct from a rotating drop-in meditation group, and the evidence base supports the former 12. If the program can specify the protocol, facilitator training, and weekly practice requirements, it's a positive indicator.
Ask how the program addresses trauma symptoms during silent practice. Dissociation, hyperarousal, and intrusive imagery are common in co-occurring caseloads. A program that hasn't considered pacing, grounding techniques, and psychoeducation for these moments is likely using a curriculum designed for a different population 6. TI-MBRP-style adaptations exist for this reason.
Determine how mindfulness is integrated with the overall treatment plan. Is it offered concurrently with CBT, DBT skills, Seeking Safety, and, when indicated, exposure-based trauma work, or is it isolated in a separate wellness track? Concurrent, integrated care aligns with VA/DoD guidance and the evidence for co-occurring conditions 1.
Two additional practical questions are crucial before making a referral: Can the program accept a warm handoff from CHAT, a detox partner, or an emergency department discharge within the first week 10? And do group times align with return service on the MAX line the individual will use 11? If the answer to either is no, the clinical model's efficacy is irrelevant if the individual cannot consistently attend.
A Note for Program Directors Managing Multiple Sites
For program directors and clinical leads overseeing multiple Portland-area locations or coordinating placements across a regional network, the operational question is not whether MBRP is effective, but whether your sites deliver it with sufficient fidelity to achieve the outcomes described in the evidence. Nine RCTs involving 901 participants demonstrated positive outcomes for craving and withdrawal under manualized conditions with trained facilitators 12. Inconsistent implementation undermines these results. When a facilitator without formal MBRP training is introduced, or when the practice duration is shortened to fit a schedule, the intervention deviates from what the trials measured, and your outcome data will reflect this before your intake numbers do.
Consider three practical steps: Standardize the curriculum across all sites so that an individual transferring between locations doesn't have to restart. Integrate facilitator supervision into your clinical calendar, beyond initial onboarding. And track PTSD symptom trajectories separately from SUD outcomes to assess the actual impact of trauma-integrated adaptations 5.
Where This Leaves the Clinician on the Referral Line
Mindfulness-based recovery in Portland is no longer a peripheral addition to co-occurring care. It is a modality with a defined evidence base for addressing craving, distress tolerance, and relapse risk, and shows promising early results for trauma symptoms when adapted for individuals with PTSD 12, 5. This does not position it as a standalone cure, nor does it replace exposure-based trauma work when clinically indicated.
What it does provide is a defensible component of a concurrent care plan for individuals with dual diagnoses, aligning with current VA/DoD guidance on integrated treatment and fitting within the structure of a Portland IOP when implemented with fidelity 1. Sequence interventions by their function. Prioritize manualized approaches. Inquire about how programs manage trauma symptoms during silent practice. If a Portland IOP like Oregon Trail Recovery is on your referral list, hold it to these same standards, allowing evidence, not marketing, to guide your decisions.
Frequently Asked Questions
Is MBRP appropriate for clients with active PTSD symptoms, or should trauma work wait until sobriety is established?
Current VA/DoD guidance rejects the older sobriety-first model. Integrated, trauma-focused care can be offered concurrently with SUD treatment, and PTSD should not gate access to either 1. MBRP is appropriate during active PTSD symptoms when the program paces silent practice carefully and handles hyperarousal with trauma-informed adaptations 6.
How does trauma-integrated MBRP (TI-MBRP) differ from standard MBRP for co-occurring PTSD-SUD clients?
TI-MBRP layers psychoeducation and elements drawn from Cognitive Processing Therapy into the standard 8-week MBRP curriculum, addressing avoidance, shame, and trauma-linked cognitions alongside core mindfulness practices 6. The 2022 RCT in women with PTSD-SUD found both TI-MBRP and standard MBRP reduced PTSD and substance use symptoms, though the authors called for confirmatory studies 5.
Where does the MBRP evidence base actually hold up, and where is it still thin?
A synthesis of nine RCTs with 901 participants shows significant effects favoring MBRP for craving and withdrawal outcomes 12. The broader mindfulness-based intervention literature is more mixed, with heterogeneity across interventions, populations, and outcome measures making clean effect sizes hard to pin down 7. Manualized MBRP has stronger footing than umbrella "mindfulness in SUD care" claims.
What should I look for in a Portland IOP that claims to offer trauma-informed mindfulness?
Ask whether the mindfulness track is manualized MBRP with trained facilitators and a defined practice arc 12. Ask how the program handles dissociation and hyperarousal during silent practice 6. Confirm concurrent sequencing with CBT, DBT, Seeking Safety, and exposure work where indicated 1. And check whether group times align with MAX and TriMet return service 11.
How does mindfulness-based recovery fit alongside CBT, DBT, Seeking Safety, and MAT in a co-occurring care plan?
Mindfulness leads on craving intensity, distress tolerance, and cue reactivity, where MBRP's mechanism data is strongest 12. It augments exposure-based trauma work like Prolonged Exposure and CPT, supporting between-session regulation rather than replacing memory processing 1. MAT and DBT skills run alongside for individuals whose clinical picture calls for pharmacotherapy or acute emotion regulation support.
Are there mindfulness-based recovery pathways in Portland for non-veteran clients and culturally specific populations?
VA Portland's Mindfulness Institute embeds groups inside SATP for veterans 3, and ODVA maintains statewide behavioral health routing 4. Non-veteran clients access community IOPs, often through CHAT/MOUD field-response handoffs 10. For Native American clients, ask how mindfulness runs alongside traditional wellness approaches like talking circles or elder-led practice rather than replacing them with a secular curriculum 8.
References
- Treatment of Co-Occurring PTSD and Substance Use Disorder in VA. https://www.ptsd.va.gov/professional/treat/cooccurring/tx_sud_va.asp
- Posttraumatic Stress Disorder and Co-Occurring Substance Use Disorders: Advances in Assessment and Treatment. https://pmc.ncbi.nlm.nih.gov/articles/PMC3811127/
- Mindfulness Institute – Veteran Programs | VA Portland Health Care. https://www.va.gov/portland-health-care/programs/whole-health/mindfulness-institute-veteran-programs/
- Behavioral Health Resources and Information – Oregon Department of Veterans' Affairs. https://www.oregon.gov/odva/resources/pages/behavioral-health.aspx
- Trauma-Integrated Mindfulness-Based Relapse Prevention for Women with Co-Occurring Post-traumatic Stress Disorder and Substance Use Disorder. https://pubmed.ncbi.nlm.nih.gov/35648046/
- Trauma-Integrated Mindfulness-Based Relapse Prevention for Women in Substance Use Treatment Settings. https://pmc.ncbi.nlm.nih.gov/articles/PMC11577492/
- Mindfulness-based interventions for substance use disorders: A systematic review and meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC8527365/
- Examining PTSD Prevalence Among Underserved Populations in Behavioral Health Care. https://pmc.ncbi.nlm.nih.gov/articles/PMC11555738/
- Substance Use Disorder Integration Report. https://www.oregon.gov/oha/HSD/AMH/DataReports/SUD-Integration-Report.pdf
- Responding to the Opioid Crisis. https://portland.gov/fire/community-health/moud-ort
- Taking public transit in Portland. https://www.portland.gov/transportation/walking-biking-transit-safety/taking-transit
- Mindfulness-based Relapse Prevention for Substance Use Disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC5636047/
Relapse Doesn't Mean the End Of Your Journey
Reach out today to explore programs that support real, long-term sobriety.




