




Benzodiazepine Addiction Treatment for Co-Occurring Disorders

Key Takeaways
- Physical dependence on benzodiazepines is an expected pharmacological response, not a use disorder — and the distinction shapes whether treatment focuses on a careful taper, relapse prevention, or both.1
- Co-occurring anxiety, PTSD, or depression drives most relapses, so treating the underlying mental health condition concurrently with the taper is the standard, not an add-on.1,7
- A safe taper means 5% to 10% dose reductions every 2 to 4 weeks with shared decision-making, never abrupt discontinuation, which risks seizures, delirium, and severe rebound symptoms.1,10
- Polysubstance use sharply raises overdose risk, with 88% of benzodiazepine-involved overdose deaths also involving opioids — making medical supervision and full honesty with prescribers essential.1,9
When the Prescription and the Diagnosis Are Tangled Together
You probably did not start taking Klonopin, Xanax, or Ativan because you wanted to. A panic attack at work, a sleepless month after a loss, intrusive memories that would not quiet down — a doctor wrote a prescription, and for a while, it helped. That is the part most people skip when they talk about benzodiazepine addiction treatment. The pill and the diagnosis came in together, and now they are hard to pull apart.
If you are reading this, you likely already know the basics. You know what your dose is. You have probably tried to cut back before and felt the rebound anxiety hit harder than the original symptom. You may have a clinician suggesting a taper while another part of you wonders what happens to the panic, the flashbacks, or the depression once the medication is gone.
That tangle is the whole problem — and the whole point of this guide. Treating the substance use side without treating the mental health condition that fueled the prescription is how relapse happens. The 2025 ASAM tapering guideline says the same thing in clinical language: address both, concurrently, or the taper does not hold.1
Physical Dependence Is Not the Same as a Use Disorder
Here is a distinction worth holding onto, because it changes how you think about what is happening in your body and what treatment actually means: physical dependence and a benzodiazepine use disorder are not the same thing. The 2025 ASAM tapering guideline is explicit about this — physical dependence is an expected pharmacological response in adults who take benzodiazepines regularly, even exactly as prescribed. Your nervous system has adapted. Stopping suddenly produces withdrawal. That is biology, not character.1
A use disorder is different. It involves loss of control over use, continued use despite harm, cravings, and the kind of behavioral patterns that pull other parts of life off course. Some people have one. Some people have both. Many people taking Klonopin or Ativan for a panic disorder or PTSD have physical dependence without meeting criteria for a use disorder at all.
Why does this matter for you? Because the framing shapes the plan. If you are dependent but not disordered, the work is a careful taper paired with treatment for the underlying mental health condition. If a use disorder is also in the picture, the plan adds relapse prevention, group support, and closer monitoring. Either way, the answer is not shame, and it is not abrupt discontinuation. It is a slower, supported path — and you get to ask which picture fits you.10
Why Co-Occurring Care Is the Rule, Not the Exception
Anxiety, PTSD, and Depression as the Engine of Relapse
If you have tried to taper before and the wheels came off, the reason is probably not weakness. It is probably the panic that came roaring back at week three, or the nightmares that returned once the medication stopped softening them. The mental health condition that put you in the prescriber's office in the first place is still there — and when the medication thins out, the condition shows up again, often louder than before.
The numbers back this up. A 2018 review of benzodiazepine misuse found that roughly 40% of people who misuse benzodiazepines also live with a comorbid psychiatric disorder. That is not a footnote. That is close to half of everyone in this situation, which means co-occurring care is not a specialty track — it is the baseline. If your treatment plan only addresses the pills and not the panic disorder, the PTSD, or the depression underneath, the plan is incomplete.7
Think about what relapse actually looks like for someone tapering off Xanax or Klonopin. It rarely starts with a craving for the drug itself. It starts with a sleepless night, a flashback in traffic, a depressive crash on a Tuesday. The pill is the answer your nervous system already knows. Treating the underlying condition — with therapy, with skills, with steady support — is how you give your nervous system a different answer to reach for.
What Long-Term Use Does to the Mental Health It Was Prescribed to Protect
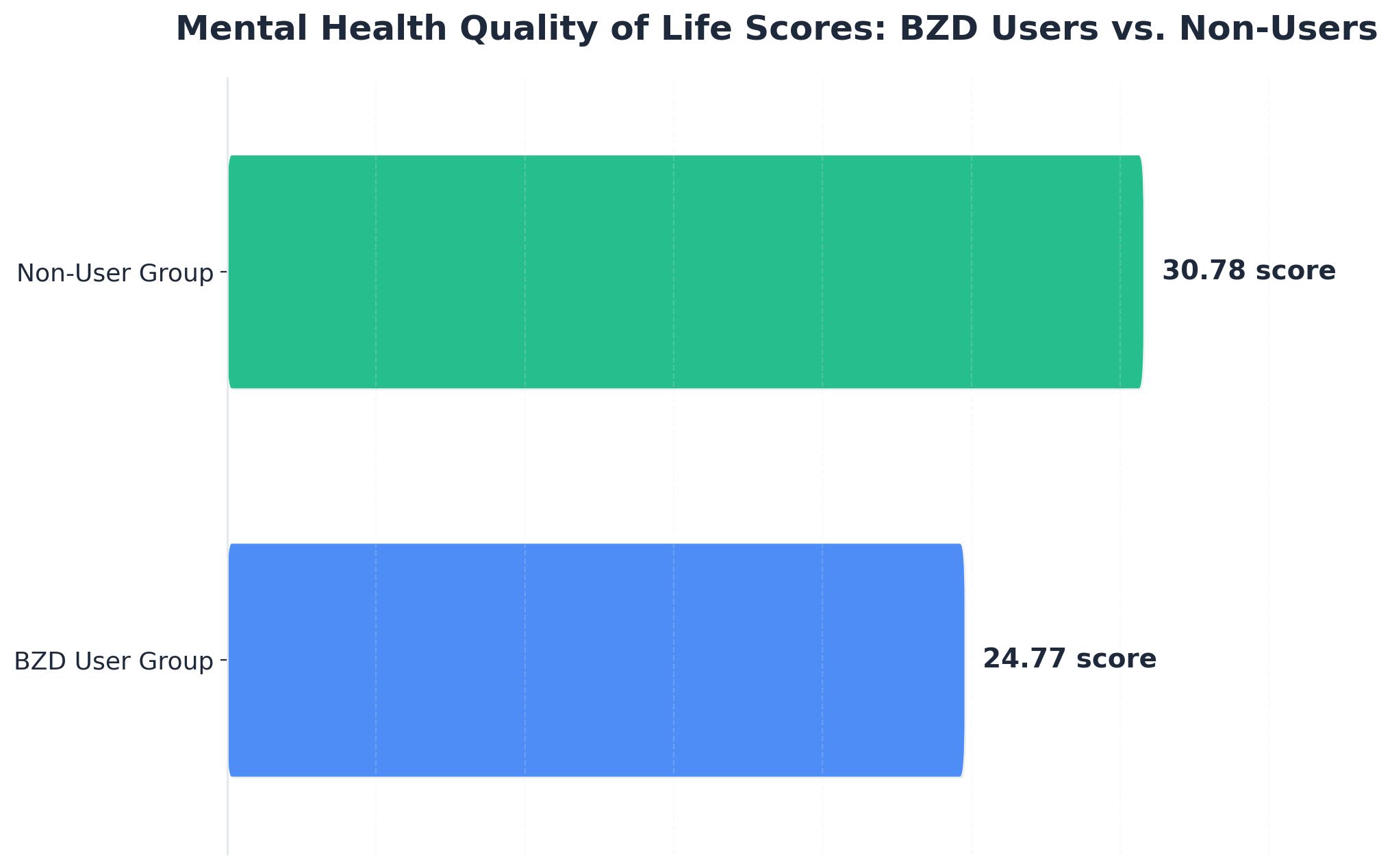
Here is the part that is hard to sit with: the medication that took the edge off in month one may be quietly making things worse by year three. A 2025 study of people with severe psychiatric disorders found that those taking benzodiazepines scored notably lower on mental health quality-of-life measures than those not taking them — 24.77 versus 30.78, a gap that reached statistical significance (p=0.030). The very symptoms the prescription was meant to ease tend to deepen with long-term use.3
That does not mean the prescription was a mistake, and it does not mean you failed. Short-term, benzodiazepines do what they are designed to do. The trouble is what happens over months and years — tolerance creeps in, sleep architecture shifts, mood flattens, cognition fogs, and the original anxiety or trauma response often becomes harder to treat, not easier. The 2019 review of co-occurring substance use and mental illness flags this same tension: benzodiazepines are effective for generalized anxiety, but the long-term picture in people with co-occurring conditions gets complicated fast.6
This is why the goal of treatment is not just stopping a medication. It is rebuilding the mental health that long-term use slowly eroded. A careful taper paired with real therapy gives you a chance to feel your baseline again — and often, that baseline is steadier than you remember.
The Tapering Math: How Slow Is Slow Enough
Pace, Dose Reductions, and Shared Decision-Making
If you have ever read a tapering schedule online and thought, "that is way too fast for what my body is doing," you were probably right. The 2025 ASAM tapering guideline puts a real number on it: an initial taper pace of 5% to 10% dose reduction every 2 to 4 weeks, and not exceeding 25% every 2 weeks even when things are going well. That is the math. It is slower than most people expect and slower than many older protocols suggested.1
Here is what that looks like in real terms. If you are taking 2 mg of Klonopin a day, a 10% reduction is 0.2 mg — and you sit at that new dose for two to four weeks before the next cut. Some people go even slower, especially after years of daily use or with a complicated mental health picture underneath. The guideline is a ceiling, not a goal. Slower is allowed. Slower is often better.
The other piece the guideline insists on is shared decision-making. That means you and your prescriber are deciding together — what dose comes off next, when, and what happens if symptoms spike. You get to say "I need another two weeks at this level" and have that count as clinical information, not as resistance. A taper that ignores how you are actually doing is a taper that tends to fail.
One more thing worth saying out loud: a slower taper is still progress. If you spent six months getting from 2 mg to 1.5 mg of Klonopin and your panic is more manageable than it was a year ago, that is the work. The pace that holds is the pace that lets your nervous system relearn how to settle without the medication doing all of it.
Why Abrupt Discontinuation Is Off the Table
Stopping benzodiazepines suddenly is not a willpower move. It is a medical risk. The 2025 ASAM guideline is clear that abrupt discontinuation can trigger withdrawal seizures, delirium, and severe rebound anxiety — outcomes that are dangerous on their own and devastating for someone already managing a co-occurring mental health condition. This is why no credible clinician will tell you to white-knuckle it.10
You may have heard stories — someone's cousin who quit cold turkey, a forum post about pushing through. What those stories usually leave out is the seizure risk, the months of protracted symptoms, and the relapse that followed when the panic or insomnia became unbearable. Your nervous system has adapted to the medication. It needs time and a structured plan to adapt back.
If you have already stopped suddenly, or someone else stopped your prescription for you, that is not a failure on your part. It is a clinical situation that needs immediate attention — usually a careful reinstatement at a lower dose followed by a proper taper. Reaching out for that kind of help is the opposite of giving up. It is the move that keeps the door open.
Detox Support and the Pacific Crest Trail Detox Partnership
Most benzodiazepine tapers happen in outpatient settings, alongside the rest of your life. Some do not. If your dose is high, your use has been long, or alcohol or opioids are also in the picture, a medically supervised detox can be the safer way to start — and the more humane one. Detox is not a punishment. It is a few days or weeks of close monitoring while your body crosses the steepest part of the curve.
For people in the Portland area and across the Pacific Northwest, that medical supervision happens through partner facilities. Oregon Trail Recovery works with Pacific Crest Trail Detox for the residential and detox piece, then steps in for the outpatient and co-occurring mental health work that follows. The hand-off matters. A detox stay that does not connect to ongoing care is where many tapers fall apart, because the pills are gone but the panic disorder, PTSD, or depression underneath has not been touched yet.
Polysubstance Risk: Benzodiazepines With Opioids or Alcohol
If benzodiazepines are in your life, and opioids or alcohol are too, the math changes. Not in a vague way. In a way that shows up in overdose statistics. The 2025 ASAM tapering guideline reports that 13.7% of opioid overdose deaths involved benzodiazepines, and 88% of benzodiazepine-involved overdose deaths also involved opioids. Read that second number again. Almost nine out of ten fatal benzodiazepine overdoses are not benzodiazepines alone — they are benzodiazepines plus something else, usually an opioid.1
Alcohol does similar damage in a different shape. SAMHSA's analysis of emergency department visits found that mixing benzodiazepines with either opioids or alcohol significantly raises the odds of a serious outcome — hospitalization, ICU admission, or death — compared to benzodiazepines on their own. Both substances are central nervous system depressants. Stack them, and breathing slows in a way the body cannot always recover from.9
If this is your situation, you are not an outlier. You are someone whose treatment plan needs to account for more than one substance at the same time. That usually means medical supervision for the early phase rather than a purely outpatient start, and it means being honest with your prescriber about everything you are taking — including the glass of wine that helps you fall asleep, or the leftover hydrocodone from a surgery last year. Honesty is not a confession here. It is clinical information that keeps you alive.
Co-occurring substance use also reshapes the taper itself. You may need to address the alcohol or opioid use first, or alongside, before the benzodiazepine reduction can move at a safe pace. That sequencing is a clinical conversation, not a willpower test — and getting it right is how the rest of the plan stays standing.
Real Recovery Starts in Portland, Oregon
Call now or verify insurance to take the first step toward lasting recovery in Portland.
Therapies That Layer On Top of the Taper
CBT for Generalized Anxiety and Panic
A taper without therapy is a recipe for the pills coming back. Cognitive behavioral therapy is the piece that gives your nervous system something else to do when the anxiety spikes — and the spikes will come, especially in the days after a dose reduction. The 2019 review of co-occurring substance use and mental illness identifies CBT as a frontline approach for the generalized anxiety and panic that often sit underneath long-term benzodiazepine use. The 2025 ASAM guideline echoes the same point: psychosocial interventions belong alongside the taper, not after it.6,10
What this looks like in practice is weekly sessions where you learn to catch the thought spirals before they become a panic attack. You practice exposure to the physical sensations — the racing heart, the tight chest — that used to send you straight to the medicine cabinet. You build a roster of skills your body can reach for at 2 a.m. instead of a half-pill of Klonopin. Slow, repeatable, unglamorous. And it works.
DBT and Trauma-Informed Care for PTSD and Emotion Dysregulation
If your benzodiazepine prescription started after trauma — a deployment, an assault, a car accident, a childhood you are still working through — CBT alone may not reach the part of your nervous system that is doing the most talking. Trauma lives in the body. Flashbacks, hypervigilance, dissociation, the 3 a.m. startle response — these need a different toolkit, one built for the kind of dysregulation that does not respond to simple thought-tracking.
Dialectical behavior therapy gives you concrete skills: distress tolerance for the moments when the wave is too big to think through, emotion regulation for the longer arc of the week, mindfulness for staying in your body when your body feels unsafe. Trauma-informed care layers on top — therapists who do not push you to retell the story before you are ready, who understand that the prescription was a coping tool, not a moral failing. The 2019 review supports this combination for co-occurring PTSD and substance use, and the 2025 guideline names psychosocial support as part of any responsible taper. You get to feel things again, slowly, with people who know what they are doing.6,10
Medication Management Without Re-Creating the Risk
You may still need medication for the anxiety, depression, or PTSD underneath — and that is fine. The work is choosing options that treat the condition without rebuilding the dependence you are trying to step away from. SSRIs and SNRIs for anxiety and depression, prazosin for trauma nightmares, buspirone for generalized anxiety — these are the kinds of tools a thoughtful prescriber considers as the benzodiazepine comes down.
One caution worth naming clearly: SAMHSA warns that combining medications used to treat substance use disorders with benzodiazepines can produce serious adverse effects. If you are also being treated for an opioid or alcohol use disorder, your prescriber needs the full picture. That is not a moment for partial honesty. It is the moment your medication list either keeps you safer or quietly stacks the risk you came in to reduce.2
What Integrated Care Looks Like in Oregon
Oregon does not treat integrated co-occurring care as a nice extra. It treats it as the floor. Oregon Administrative Rule 309-018-0160 puts it in writing: services for co-occurring mental health, substance use, and gambling disorders "shall be integrated" — meaning one plan, one team, both conditions held at the same time. The Oregon Health Authority reinforces the same expectation, naming concurrent treatment as the standard for both addictions and mental health providers across the state. If a program is sending you to one office for the Klonopin taper and a different, unconnected office for the panic disorder, that is not what Oregon means by integrated.5,8
What this looks like on a Tuesday afternoon in Portland: your therapist knows your taper schedule. Your prescriber knows what came up in last week's trauma session. The group facilitator knows you had a hard reduction on Friday and may need a quieter chair today. The information moves with you, not behind you, and the plan adjusts in real time. That coordination is the difference between a taper that holds and a taper that quietly falls apart between appointments.
For dual-diagnosis clients across the Pacific Northwest — Portland, the Willamette Valley, Central Oregon, and the rural stretches in between — integrated care also means the mental health work does not get put on hold while the substance use work happens. Both move together, week by week. That is the standard the state asks providers to meet, and it is the standard worth asking any program you are considering to describe in plain language before you sign on.
Outpatient Structure That Fits a Real Life in the Pacific Northwest
Most people doing this work cannot pause life for a month. You have a job, kids, a lease, a recovery you are trying to build into the week you already have. That is what intensive outpatient programming is built for — clinical hours that hold the weight of a real treatment plan while leaving room for the rest of your life to keep moving.
A typical IOP week in Portland looks like three to five group sessions, individual therapy, and a prescriber check-in tucked around work hours or evenings. Your CBT skills practice happens on Tuesday. Your trauma-focused work happens Thursday. Your taper adjustment gets discussed Friday before the weekend, when symptoms tend to spike. The 2025 ASAM guideline names adjunctive psychosocial interventions as a core part of any responsible benzodiazepine taper — and IOP is the structure that delivers those interventions at a clinical dose without removing you from your life entirely.10
For dual-diagnosis clients across the Pacific Northwest, this structure also makes geography workable. You can live in Gresham, Beaverton, or out toward Central Oregon and still keep a week anchored by treatment. If you are in or near Portland and looking for that kind of integrated outpatient care, Oregon Trail Recovery is one option worth a conversation.
Frequently Asked Questions
How long does a benzodiazepine taper usually take when there's a co-occurring mental health condition?
Longer than most people hope, and that is okay. The 2025 ASAM guideline recommends 5% to 10% reductions every 2 to 4 weeks, which can stretch a taper across many months — sometimes a year or more when anxiety, PTSD, or depression are also being treated. The pace that holds is the pace your nervous system can absorb without losing ground on the mental health side.1
Can I treat my anxiety, PTSD, or depression while I'm still tapering off Klonopin, Xanax, or Ativan?
Yes — and you should. The 2025 guideline calls for concurrent treatment of co-occurring psychiatric conditions during the taper, not after. CBT for panic, DBT and trauma-informed care for PTSD, and non-benzodiazepine medications for depression all run alongside the dose reductions. Waiting until the medication is gone to start mental health work is how tapers stall and relapses happen.1,6
What's the difference between physical dependence on benzodiazepines and a benzodiazepine use disorder?
Physical dependence is what your body does after regular use — your nervous system adapts, and stopping causes withdrawal. The 2025 ASAM guideline names this as expected, even with prescribed use. A use disorder is different: loss of control, continued use despite harm, cravings, life pulled off course. You can have dependence without a use disorder. The treatment plan looks different for each.1
Is it safe to stop benzodiazepines cold turkey if I want to be done with them?
No. Abrupt discontinuation can trigger withdrawal seizures, delirium, and severe rebound anxiety, which is why the 2025 guideline warns against it and calls for a structured taper with psychosocial support instead. If your prescription stopped suddenly for any reason, that is a medical situation that needs a clinician — usually reinstatement at a lower dose, then a proper taper. Reaching out is the right move.10
Does outpatient treatment in Oregon actually handle both the taper and the mental health side?
It is supposed to. Oregon Administrative Rule 309-018-0160 requires integrated services for co-occurring mental health and substance use disorders, and the Oregon Health Authority names concurrent treatment as the standard expectation across the state. In practice, that means one coordinated plan — your prescriber, therapist, and group facilitator working from the same information. Ask any program to describe how that coordination actually works.5,8
What if I'm also using opioids or alcohol along with benzodiazepines?
That changes the plan and raises the stakes. SAMHSA reports that combining benzodiazepines with opioids or alcohol significantly increases the odds of a serious emergency department outcome. Your prescriber needs the full picture — including occasional alcohol use — so the taper sequence is safe. Medically supervised detox often comes first when more than one substance is involved, followed by integrated outpatient care for the mental health work.9
References
- Joint Clinical Practice Guideline on Benzodiazepine Tapering - PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12463801/
- Co-Occurring Disorders and Other Health Conditions | SAMHSA. https://www.samhsa.gov/substance-use/treatment/co-occurring-disorders
- Benzodiazepine use and multidimensional health burden in severe psychiatric disorders. https://pmc.ncbi.nlm.nih.gov/articles/PMC12538170/
- Benzodiazepine use and abuse among patients with severe mental illness and co-occurring substance use disorders. https://pubmed.ncbi.nlm.nih.gov/14557527/
- Oregon Health Authority : Integrated Co-occurring Disorders. https://www.oregon.gov/oha/hsd/amh/pages/co-occurring.aspx
- Treatment for Substance Use Disorder With Co-Occurring Mental Illness. https://pmc.ncbi.nlm.nih.gov/articles/PMC6526999/
- Benzodiazepine use, misuse, and abuse: A review. https://pmc.ncbi.nlm.nih.gov/articles/PMC6007645/
- Or. Admin. Code § 309-018-0160 - Co-Occurring Mental Health and Substance Use Disorders. https://www.law.cornell.edu/regulations/oregon/Or-Admin-Code-SS-309-018-0160
- Benzodiazepines in Combination with Opioid Pain Relievers or Alcohol: Greater Risk of More Serious ED Visit Outcomes. https://www.samhsa.gov/data/report/benzodiazepines-combination-opioid-pain-relievers-or-alcohol-greater-risk-more-serious-ed
- Joint Clinical Practice Guideline on Benzodiazepine Tapering. https://pubmed.ncbi.nlm.nih.gov/40526204/
Relapse Doesn't Mean the End Of Your Journey
Reach out today to explore programs that support real, long-term sobriety.




