




How Rational Emotive Behavioral Therapy Helps in Portland

Key Takeaways
- REBT targets the rigid beliefs behind cravings and shame loops, teaching Portland clients to dispute thoughts like 'I can't stand this feeling' using the ABC-D-E sequence.
- Oregon expects concurrent treatment for substance use and mental health 1, making a portable cognitive skill that addresses both in the same hour especially practical inside Portland IOPs.
- Evidence shows medium effects for REBT on general outcomes and irrational beliefs 8, with gains in anxiety, depression, sleep 12, and impulse control 13— but no large RCTs for substance use disorder alone.
- Before committing to a Portland provider, compare formal REBT training versus loose CBT integration, structured ABC-D-E sessions with homework, concurrent co-occurring care, TriMet accessibility, and cultural responsiveness 10.
The Thought-Loop Problem Behind Cravings and Relapse
If you've been in recovery for any stretch of time, you already know cravings aren't just chemical. They show up wrapped in a story. "I can't stand feeling this way." "One drink won't matter." "I've already messed up today, so what's the point?" That inner monologue runs fast, often beneath your awareness, and it does real damage before you ever pick up a substance.
This is the territory Rational Emotive Behavioral Therapy was built to work in. REBT treats those automatic thoughts as learnable patterns, not character flaws. The premise is simple: the belief you hold about a hard moment, more than the moment itself, shapes what you feel and what you do next. Change the belief, and the craving loses some of its grip.
In Portland and across Oregon, that matters because most people walking into outpatient care aren't just managing substance use. They're also carrying anxiety, depression, grief, or trauma alongside it 1. The thought loop runs through all of it. Learning to interrupt that loop is one of the most practical skills you can build, and it's the heart of what the rest of this guide walks through.
What REBT Actually Does: The ABC Model and the Four Irrational Beliefs
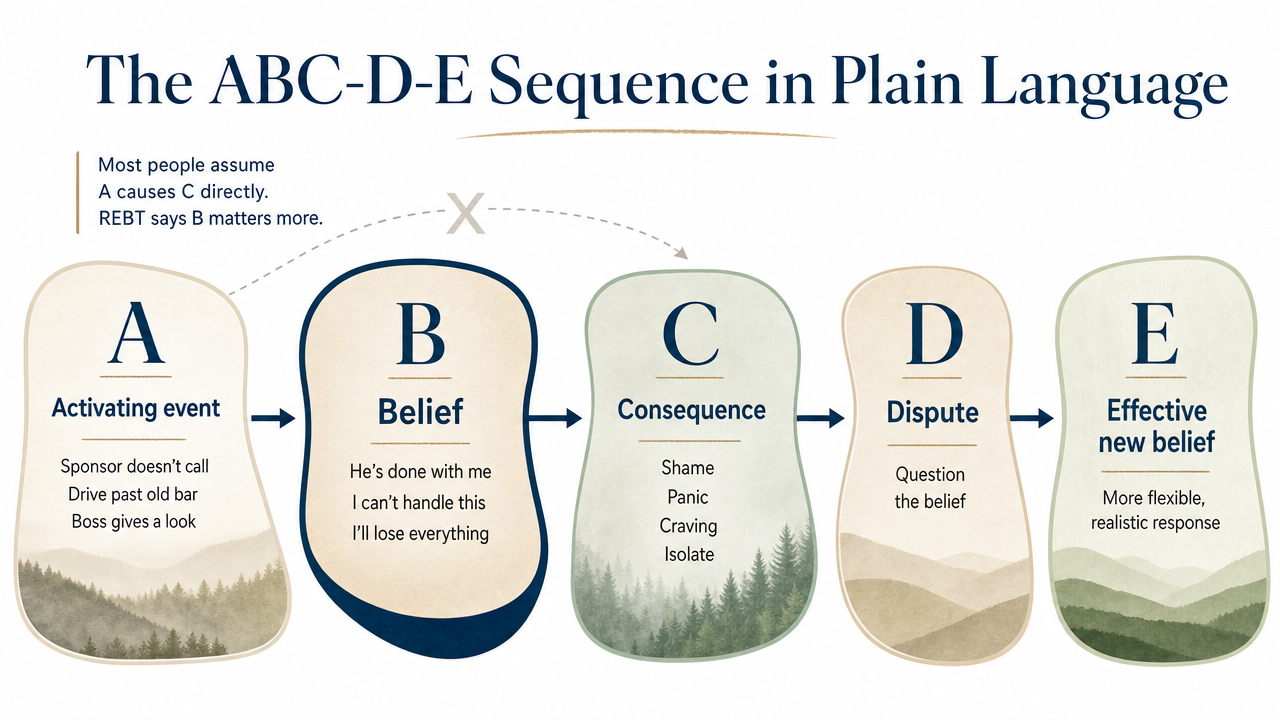
The ABC-D-E Sequence in Plain Language
Here's the framework that makes REBT different from a vague "think positive" pep talk. It's a sequence you can actually run in your head, on paper, or with a therapist sitting across from you.
- A is the Activating event.
- Your sponsor doesn't call you back. You drive past the bar where you used to spend Friday nights. Your boss gives you a look in a meeting. Something happened.
- B is the Belief you formed about it.
- This is the part most people skip. You don't usually feel the belief — it runs on autopilot. "He's done with me." "I can't handle this without a drink." "I'm going to lose this job and everything else."
- C is the Consequence
- — the feeling and the behavior that follow. Shame. Panic. A craving that feels like it came from nowhere. Maybe you isolate. Maybe you reach for something.
Most people assume A causes C directly. REBT says B is doing more of the work than you realize 7.
- D is Disputation.
- You question the belief out loud or on paper. Is it actually true your boss is firing you? Where's the evidence? Is one missed call really proof of anything?
- E is the Effective new belief
- that replaces the old one. Not a forced positive affirmation — something honest and useful. "I don't know what that look meant. I can ask, or I can let it go."
That's the loop. Activating event, Belief, Consequence, Disputation, Effective new belief. You'll practice it until it gets faster, and one day you'll catch yourself running it before a craving has time to build.
Demandingness, Catastrophizing, Low Frustration Tolerance, Depreciation
REBT-informed clinicians, including the group protocols used in VA settings for anxiety, depression, anger, and guilt, sort irrational beliefs into four recurring categories 9. Once you can name them, you can spot them faster in your own head. That's half the battle.
Demandingness is the "must" voice. I must not feel this way. My partner must understand me. I should already be over this by now. It sounds like a standard, but it's actually a rigid rule that turns ordinary disappointment into a crisis. In recovery, demandingness often shows up as "I shouldn't be having cravings anymore" — and the shame that follows feeds the very thing you're trying to step away from.
Catastrophizing is the leap to the worst-case ending. If I relapse once, my whole recovery is over. If I can't sleep tonight, tomorrow will be unbearable. The thought feels protective, like you're bracing for impact, but it actually raises your distress in the present moment for an event that hasn't happened.
Low frustration tolerance is the belief that you can't stand discomfort. This feeling is too much. I can't get through this hour. Discomfort is real. The story that you cannot survive it is not.
Depreciation is the global self-judgment. Not "I made a mistake" but "I am a mistake." Not "that was a bad choice" but "I'm broken." This one is especially heavy in recovery, where shame has often been part of the picture for years.
You'll notice these don't live in tidy lanes. A single moment can hit all four at once — you should be further along (demandingness), this proves you'll never get better (catastrophizing), you can't sit with it (low frustration tolerance), so what's wrong with you (depreciation). Learning to label them, even imperfectly, gives you something to push back against. That's the skill. And like any skill, it gets easier with reps.
REBT vs. CBT vs. DBT: A Plain-Language Contrast
You've probably seen all three letter combinations on Portland treatment websites, and it's fair to wonder what actually separates them. They're cousins, not strangers — but each one leans a different direction, and that direction matters when you're choosing where to put your energy.
REBT goes after the belief. The work is philosophical in a hands-on way. You're not just tracking thoughts; you're disputing the rigid rules underneath them — the musts, the can't-stands, the I-am-broken verdicts. REBT assumes that if you change those core beliefs, the feelings and behaviors shift downstream. It's direct, sometimes blunt, and built for repetition 7.
CBT casts a wider net. Cognitive Behavioral Therapy, the broader family REBT helped seed, works on thoughts, behaviors, and the link between them. A CBT session might spend more time on behavioral experiments, exposure work, or scheduling pleasant activities. It tends to be less focused on disputing core philosophies and more focused on testing specific thoughts against evidence. For depression and anxiety that co-occur with substance use, CBT has the deepest research base, and culturally adapted versions show meaningful results across diverse Portland communities, though effects can be somewhat smaller without thoughtful adaptation 10.
DBT plays a different position. Dialectical Behavior Therapy was built for people whose emotions hit hard and fast — intense anger, self-harm urges, relationships that swing between closeness and chaos. DBT teaches distress tolerance, mindfulness, and interpersonal skills in a structured group, alongside individual sessions. It's less about disputing beliefs and more about surviving the wave without making it worse.
In practice, Portland IOPs often weave these together. You might learn REBT's disputation skills on Monday, practice a DBT distress-tolerance skill on Wednesday, and run a CBT-style behavioral experiment by Friday. Picking a "side" isn't really the task. The task is knowing which skill fits the moment in front of you.
What the Evidence Says — and What It Doesn't
Here's the honest read on REBT research, because you deserve more than a marketing claim before you commit time and energy to a modality.
The biggest piece of evidence comes from a meta-analysis covering five decades of REBT and cognitive-behavioral therapy studies. It found a medium effect size of REBT compared to other interventions — Cohen's d = 0.58 on general outcomes at post-test, and d = 0.70 on irrational beliefs specifically 8. In plain terms: people who did REBT showed meaningful, measurable improvement, especially in the rigid thinking patterns the therapy directly targets. "Medium" isn't a small thing in therapy research. It's the range where most well-established psychotherapies land.
A more recent 2024 systematic review in PLOS One reached a similar conclusion across diverse populations: REBT consistently reduces irrational beliefs and improves outcomes like depression and anxiety 7. Other recent studies fill in the picture from different angles — improvements in anxiety, depression, and sleep quality in older adults 12, and significant gains in self-control with reductions in impulsivity in structured group settings 13. Those last two outcomes matter for recovery in obvious ways. Sleep and impulse control are not side issues; they are often the difference between a steady week and a hard one.
So what should you take from this? REBT has a credible, decades-deep evidence base for changing the thinking patterns that drive distress, and those patterns are part of what keeps cravings and shame loops running. It is not a stand-alone cure for substance use disorder, and any provider who pitches it that way is overselling. Used inside a structured outpatient program alongside other supports, it earns its seat at the table.
Why Oregon's Co-Occurring Standard Makes REBT a Practical Fit
Oregon doesn't treat substance use and mental health as two separate problems that take turns. The Oregon Health Authority is explicit about it: concurrent treatment is the expectation for both addiction and mental health providers 1. That's the standard of care. If you're walking into a Portland outpatient program with substance use and depression, or substance use and anxiety, or substance use and a trauma history, the system is supposed to address both at the same time — not send you down two separate hallways.
That policy exists for a reason, and it points directly at why a structured cognitive method earns its place in the room. Oregon's behavioral health system has documented limited capacity to actually deliver concurrent co-occurring care at the scale people need 6. When integrated care slots are tight, the modalities you do get inside an IOP have to pull more weight. They have to address mood and substance use in the same hour, with the same skill, in a way you can practice on the bus ride home.
REBT was built for that kind of double duty. The same belief that fuels a craving — I can't stand this feeling — also fuels a panic spiral or a shame loop after a hard conversation. Disputing it once gives you traction on both. That's what makes the method practical here, not theoretical. You learn one core skill, and it works on the anxiety at 3 a.m. and the craving at 6 p.m. the same way.
The Portland piece matters too. You're not just a diagnosis on a chart. You might be commuting from St. Johns, holding down a service job in the Pearl, sharing custody, or coming out of a residential stay and trying to find footing in a sober living house. A skills-based method you can rehearse between sessions fits that life better than open-ended talk therapy alone. It gives you something to do at the moment the old belief shows up — and in a city where integrated treatment capacity is still catching up to demand, having a portable tool in your pocket is not a small thing.
Real Recovery Starts in Portland, Oregon
Call now or verify insurance to take the first step toward lasting recovery in Portland.
Inside a Portland REBT Session: What the Hour Looks Like
The first ten minutes are usually quieter than you'd expect. Your therapist asks how the week landed — what came up, what you tried, where you got stuck. If you're in a group, a few people share before the work begins. Nobody's grilling you. The point of that opening is to find the moment from your week worth taking apart.
Then you pick one. Just one. Maybe it's the Sunday night before your shift, when you stood in the kitchen and felt the old pull. Maybe it's a text from someone you used to use with. Your therapist will help you slow it down and run the ABC sequence on paper or out loud — the same structure the VA uses in its manualized REBT-informed group protocol for anxiety, depression, anger, and guilt, where participants identify the activating event, the belief, the emotional and behavioral consequences, then practice disputing the belief and rehearsing a new one 18.
The middle stretch is where the real work happens. Your therapist asks pointed questions. What were you telling yourself when that text came in? Where's the evidence that you can't survive a craving without acting on it? Is that a rule, or a fact? This part can feel uncomfortable, and that's okay. You're not being argued with — you're being taught how to argue with the belief yourself, so you can do it on your own at 9 p.m. on a Tuesday.
The last fifteen minutes turn practical. You'll write down the new belief in your own words, not a clinical phrase. You'll commit to one thing to try before the next session — maybe calling a friend instead of scrolling, maybe sitting with a craving for ten minutes and timing how long it actually lasts. That homework piece is non-negotiable in REBT. The skill only gets stronger with reps.
In a Portland IOP, you'll usually do this two or three times a week, often in a mix of group and individual formats. Sessions run about an hour. By week four or five, most people start catching the belief before they catch the feeling — and the first time that happens, even once, that's a win worth naming. You did that.
Where REBT Fits in the Portland Recovery Sequence
After Detox or Residential: The IOP Handoff
The handoff out of detox or residential treatment is one of the most exposed moments in the whole recovery sequence. Your nervous system is steadier than it was a few weeks ago, but the structure around you just thinned out. The 24-hour staff, the locked schedule, the people who knew your name on day one — gone. Intensive outpatient is where most people in Portland land next, and it's where REBT really starts pulling its weight.
Here's why the timing matters. In residential, the environment did a lot of the work for you. In IOP, you're back in your apartment, back near the corner store, back inside the relationships and routines that shaped the old beliefs in the first place. The activating events come faster now. A coworker's comment. A bill in the mail. A Saturday afternoon with nothing on the calendar. Without a method for breaking those moments apart, the old loop runs unopposed.
REBT gives you something to do at that exact moment. You're not waiting for a feeling to pass on its own — you're disputing the belief that's making the feeling worse. That's why Oregon's expectation of concurrent co-occurring care matters here 1. The IOP isn't just keeping you accountable for substance use; it's teaching you a portable skill for the anxiety, anger, and shame that show up alongside it. By the time you transition out of structured outpatient, the disputation isn't a homework exercise anymore. It's a habit.
Logistics: TriMet, Work Schedules, and Sober Living Overlap
The practical layer matters more than most treatment websites admit. If you can't get to the session, the modality doesn't help you. Portland's outpatient programs sit at a workable distance from TriMet bus, MAX Light Rail, Streetcar, and Aerial Tram routes 4, which means you can build a treatment week without a car — useful if your license is on hold, if gas money is tight, or if you're sharing one vehicle with a partner.
IOP scheduling is usually built around this reality. Many Portland programs run morning, afternoon, and evening tracks so you can hold a job or stay enrolled in school. Three sessions a week, two to three hours each, is a common shape. If you're working a swing shift in the Pearl or commuting in from Gresham, ask about evening cohorts before you commit.
Sober living overlap is the other piece worth planning for. A structured house gives you the morning routine and the curfew while IOP gives you the clinical work — and REBT homework fits naturally into the quiet hours between. You can run the ABC sequence in a notebook before bed, share a tough moment in the next morning's house check-in, then bring the same moment into your therapist's office that afternoon. That repetition across settings is where the skill actually sticks. Small win, real progress.
Who Tends to Get the Most Out of REBT
REBT is not for everyone in every season of recovery, and pretending otherwise would do you a disservice. There are patterns, though, in who tends to find real traction with it.
You'll likely benefit if your inner critic runs loud and rigid. The shoulds and musts are doing a lot of damage — "I should be over this by now," "I must not feel this way in front of my family." REBT goes straight at that voice. People whose distress is fueled by perfectionism, harsh self-judgment, or all-or-nothing thinking tend to find the disputation work genuinely useful, and the research on irrational beliefs backs that up 7.
If you're working on impulse control alongside substance use, the method has real teeth. A structured REBT program with incarcerated men showed significant gains in self-control and reductions in impulsivity that held at follow-up 13. That's a population dealing with the same downstream behaviors a lot of people in recovery are working on.
If anxiety, depression, or sleep are riding alongside your substance use, REBT has shown improvement across all three in older adults 12— and those are exactly the symptoms that tend to wake cravings up at night.
Where REBT fits less cleanly: if you're in acute crisis, still in active withdrawal, or carrying untreated trauma that needs stabilization first. The directness of the disputation can feel like too much, too soon. That's not a failure on your part — it's a sequencing question your clinician can help you sort out. For Portland's diverse communities, the cognitive therapy family works, though the research is honest that thoughtful cultural adaptation makes the work land better 10. Ask about that fit early. You deserve a therapist who meets you where you actually live.
Choosing a Portland Provider: Questions Worth Asking
Not every provider listing REBT on a website is actually trained in it, and you have every right to ask. A short phone call before you commit can save you weeks.
Start with the basics. Is REBT one of the modalities your clinicians are formally trained in, or is it something woven loosely into general CBT work? Both can be useful, but you deserve a straight answer. Ask whether sessions follow a structured format — activating event, belief, disputation, new belief — or whether the work stays in open conversation.
Then go to fit. How do you handle co-occurring conditions in the same treatment plan? Oregon's standard expects concurrent care for substance use and mental health 1, so the answer should be specific, not vague. Ask about cultural responsiveness too — cognitive therapies work across diverse communities, but thoughtful adaptation matters 10.
Finally, the practical layer. What does the IOP schedule look like around work or school? Is the location reachable by TriMet or MAX? Is there a sober living connection if you need that bridge? A good provider will answer these without flinching — and if they do, you've likely found a place worth showing up for.
Frequently Asked Questions
Is REBT different from CBT, or is it the same thing?
They're related, not identical. REBT is one of the founding therapies in the CBT family and shares the same core idea — thoughts shape feelings and behavior. The difference is focus. REBT goes hard at the rigid core beliefs underneath your thoughts (the musts, the can't-stands) and disputes them directly. Broader CBT often spends more time on behavioral experiments and testing specific thoughts against evidence 7.
Can REBT replace medical detox or residential treatment?
No, and any provider telling you otherwise is overselling. REBT is a skills-based outpatient therapy, not a medical intervention. If you're in active withdrawal or your use pattern is unsafe to stop on your own, you need medical detox first. REBT earns its place after stabilization, inside an IOP or step-down program, as one tool within a broader recovery plan.
How long does it take to see results from REBT?
Most people start catching the belief before the feeling around weeks four to six of regular practice — sometimes sooner. The meta-analytic evidence shows medium effects at post-treatment, meaning real, measurable change happens during a typical course of therapy, not years later 8. The honest piece: the skill keeps deepening with reps. Early wins are real, and they build.
Does REBT work for co-occurring anxiety, depression, or trauma alongside substance use?
Yes, with some caveats. REBT has documented improvements in anxiety, depression, and sleep 12, and REBT-informed group protocols are used in VA settings for co-occurring anger, guilt, depression, and anxiety 18. For active trauma, the directness of disputation can feel like too much without stabilization first. A good clinician will sequence the work — stabilize, then layer in the cognitive piece. That's the standard concurrent-care expectation in Oregon 1.
Can I do REBT over telehealth, or do I need to go in person in Portland?
Both work. REBT's structured, homework-driven format translates well to video sessions, and research on telehealth-delivered cognitive therapies shows symptom improvements in real-world cohorts 19. Many Portland IOPs offer hybrid schedules — some group days in person, individual sessions remote. If transit is a barrier, telehealth keeps you in the work. If your home environment is unsteady, in-person can offer the structure you need.
What should I ask a Portland therapist to know if they really practice REBT?
Ask three things. First, are clinicians formally trained in REBT, or is it folded loosely into general CBT? Second, do sessions follow the ABC-D-E structure with written homework between meetings? Third, how does the program handle substance use and mental health symptoms in the same plan — Oregon expects concurrent care 1. Specific answers signal real practice. Vague ones tell you to keep looking.
References
- Oregon Health Authority : Integrated Co-occurring Disorders. https://www.oregon.gov/oha/hsd/amh/pages/co-occurring.aspx
- National Survey on Drug Use and Health: 2023 State-Specific Tables – Oregon. https://www.samhsa.gov/data/sites/default/files/reports/rpt56188/2023-nsduh-sae-state-tables_0/2023-nsduh-sae-state-tabs-oregon.pdf
- Portland city, Oregon - U.S. Census Bureau QuickFacts. https://www.census.gov/quickfacts/fact/table/portlandcityoregon/IPE120224
- Taking public transit in Portland. https://www.portland.gov/transportation/walking-biking-transit-safety/taking-transit
- Behavioral Health Unit | Portland.gov. https://www.portland.gov/police/divisions/behavioral-health-unit
- COD Service Inventory 2022. https://www.oregon.gov/oha/HSD/AMH/DataReports/COD-Service-Inventory-2022.pdf
- A systematic review of the nature and efficacy of Rational Emotive Behaviour Therapy (REBT). https://pmc.ncbi.nlm.nih.gov/articles/PMC11232995/
- 50 years of rational-emotive and cognitive-behavioral therapy: A systematic review and meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC5836900/
- A Narrative Commentary on the Use of a Rational Emotive Behavior Therapy-Informed Group for Veterans With PTSD. https://pmc.ncbi.nlm.nih.gov/articles/PMC10886947/
- Culturally Responsive Cognitive Behavioral Therapy for Ethnically Diverse Populations. https://pubmed.ncbi.nlm.nih.gov/36854287/
- Rational emotive intervention for work-family conflict and female academics. https://pmc.ncbi.nlm.nih.gov/articles/PMC9476453/
- Effects of rational emotive behavior therapy on alexithymia, anxiety, depression and sleep quality of older people. https://pmc.ncbi.nlm.nih.gov/articles/PMC10463404/
- Effectiveness of Rational Emotive Behavior Therapy (REBT) on Self-Control and Impulsivity in Male Prisoners. https://pmc.ncbi.nlm.nih.gov/articles/PMC11055976/
- The effectiveness of rational emotive behavior therapy (REBT) and mindfulness in athletes. https://pmc.ncbi.nlm.nih.gov/articles/PMC10724889/
- State of Housing in Portland 2024 - Executive Summary. https://www.portland.gov/phb/documents/state-housing-portland-2024-executive-summary/download
- III.B. Overview of the State - Oregon - 2024. https://mchb.tvisdata.hrsa.gov/Narratives/Overview/08657c19-0041-4a79-aea2-657ec67ce181
- Rational-emotive and cognitive-behavior therapy (REBT/CBT) versus pharmacotherapy versus REBT/CBT plus pharmacotherapy in the treatment of major depressive disorder in youth: a randomized clinical trial. https://pubmed.ncbi.nlm.nih.gov/25500320/
- Rational Emotive Behavior Therapy-Informed Treatment for Anxiety and Depression: Patient Workbook. https://www.mirecc.va.gov/visn6/Docs/0987_RICVA_REBT_PatientWkbk_F2b_508_compliant.pdf
- Real-world patient outcomes for telehealth-delivered, remote eating disorder treatment: a systematic review. https://pmc.ncbi.nlm.nih.gov/articles/PMC12613931/
Relapse Doesn't Mean the End Of Your Journey
Reach out today to explore programs that support real, long-term sobriety.




